Home » Counselor Intern (Page 7)
Category Archives: Counselor Intern
The First Interview – Addictions Counseling
1. Goals in a first interview
a. Allow the client to tell you her/his story in her/his own words
b. Let the client know that you understand what she/he believes, even when it includes that she/he does not need to be there.
c. This is not the moment to express that you may disagree with client.
2. The first interview with the self-referred adult
a. The client feels the need to explore the possibility of getting therapy.
3. Prepare yourself in advance
a. Has the client been in the therapy before?
b. Review documentation
- Medical history
- Psychiatric evaluation
- Biopsychosocial assessment
- Previous clinician’s notes
c. Ask yourself
- What don’t I know that I need to know?
- Write down notes and questions you want to ask before calling the client to set up an appointment
- Add a healthy dose of skepticism to everything you find out
4. What to ask your supervisor before the first interview
a. Any questions you have after reading documents provided on the client
b. Whom to include in the interview
c. How long the session should last
d. How often should you see the client
e. How to introduce your self
f. When and how to record sessions
5. When calling the client, remember that
a. Your relationship with the client starts right there
b. How should you introduce yourself to the client
c. Be professional and concerned
d. Remember that this is NOT a therapy session
e. Maintain confidentiality from this moment on
- Find out if, and under what circumstances, you are required by law not to maintain confidentiality.
- Except in those circumstances (above), always get written consent from the client to share identifying information to other agencies
- Telephone calls: remember that even the fact that the individual is a client is confidential information.
- When necessary use fictious names and situations
6. The room set up is important
a. Keep it comfortable and simple
b. How would YOU feel coming here?
7. Before you start the interview
a. Select an assessment instrument, based on
- Your agency
- The age of the client
- Reliable
- Valid
b. Explain the assessment process to the client
8. Ask your supervisor how you should gather information during the session
a. Taking notes?
b. Just listening?
c. Audiotaping?
d. Videotaping?
e. Using a computer?
9. During the interview/session
a. Start where the client is
b. Your concern is the client’s feelings
c. Keep self-disclosure to the minimum
d. The focus is on the client, not on you
e. Practice active listening
f. Do not put words or feelings into your client’s mouth
g. Ask who, what, when, where, and how
h. Don’t ask WHY
- It assumes client knows the answer to his/her problem
- Client might feel attacked and therefore act defensive
- They might tell you more than they are ready to share
- If client tells you more than they meant to, they might never come back
10. Presenting problem
a. Why is the client here now?
- Basic data
11. At the end of the session
a. Leave enough time to ask your client if there are any questions
b. Ask client if she/he would like to come back
c. Give the client a card with information about her/his next appointment
d. Walk your client to the door
e. Be aware of the door-knob syndrome
- Client waits to tell you something very important until there is not time left to discuss it
- You can end the session by saying “That sounds like something we should talk about. Let’s begin with that next week.”
- You NEVER let a client leave your office if you have a sense that she/he might hurt her/himself or others.
Reference: Where to Start and What to Ask – Susan Lukas

Addiction Counseling Tools: The MSE – Mental Status Exam
The Mental Status Exam (MSE)
- It is the process of noting the observable in some systematic way
- It is different from the biopsychosocial assessment
- Based mostly on facts about the client’s life
- Description of the problem provided by the client
- The MSE is basically our observations
- It’s a very useful tool for assessing a client over time
2. Helpful questions for the MSE
- What has changed?
- When did it change?
- Has it change for the better or the worse?
- Ask for further explanation when you don’t understand something the client has told you
- Document what is worth noting
- Start by describing those things that anyone looking at the client would notice
- It does not matter when the MSE is completed
- Remember that a good clinician is a good observer
- To infer meaning from what you are actually seeing
- To see things that are in reality just your assumptions
- Appearance
- How does the client look and behave?
- Speech
- How does the client speak?
- Emotions
- What is the client’s mood/affect?
- How does the client feel most of the time?
- How does the client appear to be feeling during the interview with you?
- Thought process and content
- How does the client think?
- Circumstantiality – takes a while to get to the point
- Perseveration – repeating phrase or returning to same subject
- Association – how does the client get from one idea to the next?
- How does the client think?
- What does the client think about?
- Delusions?
- Compulsions?
- Sensory perception
- Illusions?
- Hallucinations?
- Mental Capacities
- Is the client oriented in time, place, and person?
- What is your estimate of the client’s intellingence?
- Can the client remember and concentrate?
- How are the client’s judgment and insight?
- Attitude toward the interviewer
- Client’s attitude towards you
- Does it change over time?
- Does he/she respond to empathy?
- Does he/she appear to be capable of empathy?
Reference: Where to Start and What to Ask – Susan Lukas. (This is by far one of my favorite books. I highly recommend it)
Dual Disorders – David O’Connell
Drug Addiction and Co-occurring Disorders
-
Co-Occurring Disorders
-
Substance abuse problems combined with mental disorders
-
Counselors/therapists can treat clients with co-occurring disorders by mastering basic approaches
-
-
Models of Training
-
Scientific Professional Model
-
Training of psychologists and psychiatrists
-
Classroom teaching of “facts”
-
-
- Craft Model
- Traditional addictions counseling training
- Based on personal experience and on-the-job apprentice-style training and supervision
There advantages and disadvantages of both, but can be overcome by combining them.
- First Steps
- Learn about the disorder
- Read available literature on the topic
- DSM-IV
-
Assess the client carefully
- Avoid misdiagnosing clients due to overlapping of symptoms between the effects of a drug and a mental disorder
- Is there a mental disorder, regardless of the substance abuse problem?
- Is the substance causing the symptoms? (e.g. schizophrenia, paranoia, depression due to substance use)
-
Learn what to avoid in treatment
- Do no harm
-
Learn appropriate treatment strategies
- Continuing Care
- Help the client maintain sobriety and the mental disorder under control by providing good after-care.
- Role of Medication
- Become familiar with the client’s medication
- Medication should be monitored closely
Psychiatric and Psychological reports
- Impulse control
- Client’s tendency to act on feelings, thoughts, or impulses
-
Level of functioning
-
How well clients manage their impulses
-
-
Affective expression
-
Client’s style of emotional expression
-
-
Cognitive functioning
-
Client’s level of intelligence
-
-
Perceptual functioning
-
Nature and frequency of client’s perceptual disturbances
-
-
Reevaluation
-
Avoid undermining treatment
-
Encourage AA or NA involvement
-
Supervision
-
Well-trained addictions therapists/counselors can skillfully treat the psychiatric disorder and the substance abuse disorder
-
Competence in the brief therapies is needed
-
Cognitive Behavioral Therapy (CBT) is one of the most effective ones.
Reference: Dual Disorders – David F. O’Connel
Rational Emotive Behavior Therapy (REBT) – Albert Ellis
1. View of Human Nature
a. REBT assumes that the individual has the capacity to be completely rational, irrational, sensible or crazy, which Ellis believed is biologically inherent .
b. Ellis was most concerned with irrational thinking especially that which creates upsetting or irrational thoughts.
c. Most common irrational beliefs that clients find disturbing (Ellis, 1984, p.266)
i. It is absolutely essential to be loved or approved of by every significant person on one’s life.
ii. To be worthwhile, a person must be competent , adequate, and achieving in everything attempted.
iii. Some people are wicked, bad, and villainous and therefore should be blamed or punished.
iv. It is terrible and a catastrophe whenever events do not occur as one hopes.
v. Unhappiness is the result of outside events, and therefore a person has no control over such despair.
vi. Something potentially dangerous or harmful should be cause to great concern and should always be kept in mind.
vii. Running away from difficulties and responsibilities is easier than facing them.
viii. A person must depend on others and must have someone stronger on whom to rely.
ix. The past determines one’s present behavior and thus cannot be changed.
x. A person should be upset by the problems and difficulties of others.
xi. There is always a right answer to every problem, and a failure to find this answer is a catastrophe.
d. Individuals are easily disturbed because of gullibility and suggestibility
e. Ellis was a proponent of the individual thinking of their behavior as separate from their personhood, i.e. “I did a bad thing” rather than “I am a bad person.”
f. Ellis believed that each individual has the ability to control their thoughts, feelings and their actions. In order to gain this control, a person must first understand what they are telling themselves (self-talk) about the event or situation .
g. Cognitions about events or situations can be of four types: positive, negative, neutral, or mixed. These cognitions result in similar thoughts with positive leading to positive thoughts, negative leading to negative thoughts, etc.
2. Role of the Counselor
a. Counselors are direct and active in their teaching and correcting the client’s cognitions.
b. A good REBT counselor must be bright, knowledgeable, empathetic, persistent, scientific, interested in helping
others and use REBT in their personal lives (Ellis, 1980).
c. The counselor does not rely heavily on the DSM-IV categories.
3. Goals
a. The primary goal is to help people live rational and productive lives.
b. REBT helps people see that it is their thoughts and beliefs about events that creates difficulties, not the events or situations themselves
c. REBT helps the client to understand that wishes and wants are not entitlements to be demanded. Thinking that involves the words must, should, ought, have to, and need are demands, not an expression of wants or desires.
d. REBT helps clients stop catastrophizing when wants and desires are not met
e. REBT stresses the appropriateness of the emotional response to the situation or event. An situation or event need not elicit more of a response than is appropriate
f. REBT assists people in changing self-defeating behaviors or cognitions
g. REBT espouses acceptance and tolerance of self and of others in order to achieve life goals
4. Techniques
a. The first few sessions are devoted to learning the ABC principle:
i. Activating event
ii. Belief or thought process
iii. Emotional Consequences
b. Cognitive disputation is aimed at asking the client questions challenging the logic of the client’s response.
c. Imaginal disputation has the client use imagery to examine a situation where the become upset. The technique is used in one of two ways:
i.The client imagines the situation, examines the self-talk, and then changes the self-talk leading to a more moderate response.
ii.The client imagines a situation in which they respond differently than is habitual, and are asked to examine the self-talk in this
imagery.
d. The Emotional Control Card is an actual card intended for the client to carry in their wallet which has a list of inappropriate or self-destructive feelings countered with appropriate nondefeating feelings. In a difficult situation, the client has this reference card on their person to help them intervene in their own self-talk. (source: http://www.liverehab.com/rational-emotive-behavioral-therapy)
e. Behavioral disputation involves having the client behave in a way that is opposite to the way they would like to respond to the event or situation.
f. Confrontation occurs when the counselor challenges an illogical or irrational belief that the client is expressing.
g. Encouragement involves explicitly urging the client to use REBT rather than to continue self-defeating responses.
Study Materials: Learn About the Addiction Counseling Field
Hello dear readers and subscribers,
This is just a quick reminder of the new study materials available for you to download, print, share, etc…
Visit the Downloads page to download documents in pdf.
Visit the Resources page for suggested textbooks, websites, videos, and more…all about the substance abuse counseling field.
Visit the Online Quizzes for links to practice quizzes. No passwords or any other requirements are needed.
Visit the home page (click on header image) to check out the headlines of my posts from my other blogs.
Remember: The study guide for IC&RC ADC exam will be moved to my Blogger blog http://lcdcecstudyguide.blogspot.com/. The WordPress blog (the one you are reading right now) will still have some of the previous content from the study guide. However, I will publish many other things that are not included on the test.
I hope this is helpful. Feel free to contact me with any questions and suggestions you have.
Counselor Developmental Levels
From one of my favorite SAMHSA Publications
TIP 52 – Clinical Supervision and Professional Development of the Substance Abuse Counselor
Each counselor goes through different stages of development. The movement through these stages is not always linear and can be affected by changes in assignment, setting, and population served.
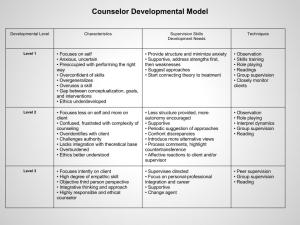
Go to my Downloads page to download this table and TIP 52.
Effective Counseling Skills
Shared by contributor Yvette McBride Thomas
Hello everybody!
Here is the pdf document that you can download.
Effective Counseling Skills
Let me know if you have any problems downloading the document.
Good day!
