Home » Articles posted by Samantha DeLint-Neely (Page 11)
Author Archives: Samantha DeLint-Neely
Study Materials: Learn About the Addiction Counseling Field
Hello dear readers and subscribers,
This is just a quick reminder of the new study materials available for you to download, print, share, etc…
Visit the Downloads page to download documents in pdf.
Visit the Resources page for suggested textbooks, websites, videos, and more…all about the substance abuse counseling field.
Visit the Online Quizzes for links to practice quizzes. No passwords or any other requirements are needed.
Visit the home page (click on header image) to check out the headlines of my posts from my other blogs.
Remember: The study guide for IC&RC ADC exam will be moved to my Blogger blog http://lcdcecstudyguide.blogspot.com/. The WordPress blog (the one you are reading right now) will still have some of the previous content from the study guide. However, I will publish many other things that are not included on the test.
I hope this is helpful. Feel free to contact me with any questions and suggestions you have.
Counselor Developmental Levels
From one of my favorite SAMHSA Publications
TIP 52 – Clinical Supervision and Professional Development of the Substance Abuse Counselor
Each counselor goes through different stages of development. The movement through these stages is not always linear and can be affected by changes in assignment, setting, and population served.
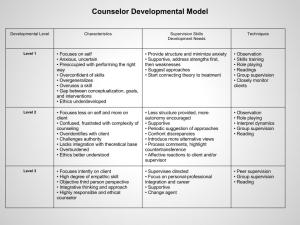
Go to my Downloads page to download this table and TIP 52.
Effective Counseling Skills
Shared by contributor Yvette McBride Thomas
Hello everybody!
Here is the pdf document that you can download.
Effective Counseling Skills
Let me know if you have any problems downloading the document.
Good day!
Your Recovery Plan – Nutrition Is Key
12 Steps; support groups; counseling; do-this-not-that…all this is important during substance abuse recovery but, what about a good nutrition?
Have you noticed that most people get angry, moody, or depressed when they are hungry and don’t eat for several hours? This is a natural response when our body is being deprived from the nutrients it needs. A good nutrition is especially important during recovery from substance abuse. Feelings of sadness, anger, frustration, and hunger can be triggers for a potential relapse. We don’t think about it this way but when we are hungry our body is needing something, is asking for something. Many times people get rid of these sensations by using alcohol or drugs, so they don’t have to feel hungry anymore. During recovery, the body continues to crave not only basic things such as food, water, and sex (basic needs) but also the cravings for the drug of choice.
Your recovery plan. We don’t have to be dietitians or nutritionists,

nor do we want to pretend to be one, to advice our clients that a proper nutrition is key during recovery from addiction. Just as we advice them to go to 12 Step-meetings, support groups, and counseling, we can also advice them to add an exercise routine and a proper nutritious diet to their recovery plan.
Break the cycle. Keep in mind that the brains of substance abusers have been conditioned to seek pleasure and avoid pain. The pleasure seeking behavior is the craving for the drug. If your diet is based on junk food, sodas, and sweets, you are only feeding the cycle of addiction, not your body!
Anyone, whether they suffer from addiction or not, experiences a form of depression, weakness, and lack of motivation when they are deprived from food. People in recovery can prevent a relapse by paying attention to HALT: avoid getting too hungry, angry, lonely, or tired, because these could be triggers.
Here is an article from my blog about recovery and wellness coaching. Thanks for reading!
Aloe Miracle Nutrition: Recovery And Wellness Through Nutrition.
8 Practice Domains of Substance Abuse Counselors
8 Practice Domains – 137 Questions on the IC&RC ADC Exam
Domain 1: Clinical Evaluation – 24 questions
• Discuss with the client the rationale, purpose, and procedures associated with the screening and assessment process to facilitate client understanding and cooperation.
• Assess client’s current situation, including signs and symptoms of intoxication and withdrawal, by evaluating observed behavior and other available information to determine client’s immediate needs.
• Administer the appropriate screening and assessment instruments specific to the client’s age, developmental level, culture, and gender in order to obtain objective data to further assess client’s current problems and needs.
• Obtain relevant history and related information from the client and other pertinent sources in order to establish eligibility and appropriateness to facilitate the assessment process.
• Screen and assess for physical, medical, and co-occurring disorders that might require additional assessment and referral.
• Interpret results of data in order to integrate all available information, formulate diagnostic impressions, and determine an appropriate course of action.
• Develop a written summary of the results of the assessment in order to document and support the diagnostic impressions and treatment recommendations.
Domain 2: Treatment Planning – 20 questions
• Formulate and prioritize mutually agreed upon problems, immediate and long-term goals, measurable objectives, and treatment methods based upon assessment findings for the purpose of facilitating a course of treatment.
• Use ongoing assessment and collaboration with the client to review and modify the treatment plan to address treatment needs.
Domain 3: Referral – 10 questions
• Match client needs with community resources considering client’s abilities, gender, sexual orientation, developmental level, culture, ethnicity, age, and health status to remove barriers and facilitate positive client outcomes.
• Identify referral needs differentiating between client self-referral and direct counselor referral.
• Explain to the client the rationale for the referral to facilitate the client’s participation with community resources.
• Continually evaluate referral sources to determine effectiveness and outcome of the referral.
Domain 4: Service Coordination – 10 questions
• Communicate with community resources concerning relevant client information to meet the identified needs of the client.
• Advocate for the client in areas of identified needs to facilitate continuity of care.
• Evaluate the effectiveness of case management activities through collaboration with the client, treatment team members, and community resources to ensure quality service coordination.
• Consult with the client, family, and concerned others to make appropriate changes to the treatment plan ensuring progress toward treatment goals.
• Prepare accurate and concise screening, intake, and assessment documents.
Domain 5: Counseling – 33 questions
• Educate the client regarding the structure, expectations, and limitations of the counseling process.
• Utilize individual and group counseling strategies and modalities to match the interventions with the client’s level of readiness.
• Continually evaluate the client’s level of risk regarding personal safety and relapse potential in order to anticipate and respond to crisis situations.
• Apply selected counseling strategies in order to enhance treatment effectiveness and facilitate progress towards completion of treatment objectives.
• Adapt counseling strategies to match the client’s needs including abilities, gender, sexual orientation, developmental level, culture, ethnicity, age, and health status.
• Assist families and concerned others in understanding substance use disorders and utilizing strategies that sustain recovery and maintain healthy relationships.
• Document counseling activity to record all relevant aspects of treatment
Domain 6: Client, Family, and Community Education – 15 questions
• Provide education on issues of cultural identity, ethnic background, age, sexual orientation, and gender in prevention, treatment, and recovery.
• Provide education on health and high-risk behaviors associated with substance use, including transmission and prevention of HIV/AIDS, tuberculosis, sexually transmitted infections, hepatitis, and other infectious diseases.
• Provide education on life skills, including but not limited to, stress management, relaxation, communication, assertiveness, and refusal skills.
• Provide education on the emotional, cognitive, and behavioral aspects of substance use to develop an understanding of the psychological aspects of substance use, abuse, and addiction.
• Provide education on the sociological and environmental effect of substance use to develop an understanding of the impact of substance use on the affected family systems.
• Provide education on the continuum of care and resources available to develop an understanding of prevention, intervention, treatment, and recovery.
Domain 7: Documentation – 17 questions
• Obtain written consent to release information from the client and/or legal guardian, according to best practices and administrative rules, to exchange relevant client information with other service providers.
• Document treatment and continuing care plans that are consistent with best practices and applicable administrative rules.
• Document client’s progress in relation to treatment goals and objectives.
• Prepare accurate and concise reports and records including recommendations, referrals, case consultations, legal reports, family sessions, and discharge summaries.
• Document all relevant aspects of case management activities to assure continuity of care.
• Document process, progress, and outcome measurements.
Domain 8: Professional and Ethical Responsibilities – 21 questions
• Adhere to jurisdictionally-specific rules and regulations regarding best practices in substance use disorder treatment in order to protect and promote client rights.
• Recognize individual differences of the counselor and the client by gaining knowledge about personality, cultures, lifestyles, gender, sexual orientation, special needs, and other factors influencing client behavior to provide services that are sensitive to the
uniqueness of the individual.
• Continue professional development through education, self-evaluation, clinical supervision, and consultation in order to maintain competence and enhance professional effectiveness.
• Identify and evaluate client issues that are outside of the counselor’s scope of practice and refer to other professionals as indicated.
• Advocate for populations affected by substance use and addiction by initiating and maintaining effective relations with professionals, government entities, and communities to promote availability of quality services.
• Apply current counseling and psychoactive substance use research literature to improve client care and enhance professional growth.
Reference: IC&RC Candidate Guide
Re-blogged from LCDC Exam Review (WordPress)
LCDC Exceptional Counselor Study Guide – Get Ready With Me
Hello readers and subscribers!
I invite you to visit and subscribe to the new blog/study guide LCDC Exceptional Counselor Study Guide (link below). Keep reading to know why 😉
What’s the difference between the two?
LCDC Exceptional Counselor Study Guide (new blog) will publish information exclusively to prepare for the IC&RC ADC exam. I will follow the IC&RC Candidate’s Guide to make sure that only relevant information for the exam gets published here. Visit the new blog to learn more about the structure of the IC&RC certification exam.
LCDC Exam Review will continue to publish information for all things substance abuse counseling. All this knowledge is good to have, but a lot of these things are not going to be included on the certification exam such as research articles on addiction science or the topics discussed in the internship/classes forum. LCDC Exam Review will post announcements (when necessary) and reblogs on articles that I consider worth reading to enhance our understanding of addiction and addiction counseling. So, as you can see, this is a lot of information that doesn’t need to be on the study guide.
Come check it out and stay tuned to the upcoming posts for the areas that cover the IC&RC exam study guide.
Thanks and see you soon!
Samantha DeLint
LCDC Exceptional Counselor Study Guide – Get Ready With Me.
Marijuana – Understanding Addiction
 • Marijuana is a leafy material from the cannabis plant that is smoked.
• Marijuana is a leafy material from the cannabis plant that is smoked.